Although the surgical procedures is not the focus of this blog, I would like to share with everyone a new technique that we are performing in our practice. The majority of ankle sprains do not require surgical treatment. In fact, most athletes are able to return to running and competition within 2-3 weeks of an acute ankle sprain. Even a severe sprain can go on to an almost normal recovery. Sometimes however, the condition becomes chronic which typically occurs over several years. One usually encounters sprains of the ankle by just stepping of a curb the wrong way, or even periodically during a season of competition. When this occurs, your ankle may be inhibiting you from performing the activities you otherwise would be able to do. Surgery is usually indicated at this point.
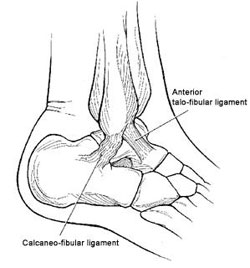
In the past, surgery typically involved a primary repair (tightening of the ligament itself) or a secondary repair (utilizing the patients own tendons to recreate a ligament). While these procedures work well, they do have some complications. The primary repair which involves tightening the ligament itself, is only as strong as the ligament that remains.

Primary repair where suture is used to tighten the ligaments.
There are numerous variations of secondary repair most of which involve harvesting a portion of the peroneous longus tendon and using it to augment and/or recreate the ATF and CF ligaments. When the peroneous tendons are sacrificed for utilization in repairing the ligaments, the tendon itself has to undergo a healing and repair process adding to further swelling and pain post operatively. In essence, not only does the ligament repair need time for healing, the disrupted tendon now has to heal and repair. It’s almost as if the patient is healing two procedure instead of one.

Secondary repair involving harvesting a peroneal tendon for recreation of the lateral ligamentous complex.
The technique performed on the patient in the video below involved recreating of the ATFL and CFL with the use of a product known as Fibertape by Arthrex. Fibertape is an ultra-high strength suture material that is anchored into the bone at the sites corresponding to the attachments of the ligaments. A corkscrew anchor provides a tight fit resisting the ability to be pulled out. The Fibertape is described by Arthrex as being an augmentation to the existing ligament, but in actuality it is much stronger then the body’s own ligament tissue and provide more support then just augmenting the ligament itself.

Fibertape and Tigertape by Arthrex

Augmentation of a primary repair with the Arthrex Fibertape
See the video below revealing the improvement in strength of the ligaments and minimal swelling at just 3 weeks post operatively.

My blog has been in existence now for almost one year. I started it after speaking to someone on a plane after returning from a lecture I gave on running at Vibram USA. This person was fascinated about what I was doing with FiveFingers and the success I was having at transitioning runners into more minimalist shoes. They wanted to read more about what I was doing and if I wrote a blog. It didn’t exist. Thus began Dr. Nicks Running Blog. The goal was to spread the word about minimalist running shoes and the site has since evolved into all aspects of running. Many runners have reached out to me with their problems and questions, and it has been amazing to be able to help them by providing information here. I have even had patients travel several hours to be seen for issues more complex then could be solved by simply “reading” on the site. I’ve received tons of stories from runners who have transitioned to minimalist shoes and resolved a chronic injury.
As a thank you, as well as to spread the word on some of these fascinating stories, we are giving away a pair of Vibram FiveFingers to the “most unique” or “successful” story to a runner or non runner who has resolved an injury by transitioning out of traditional running shoes and into minimalist shoes. The story will be featured on Dr. Nick’s Running Blog which is read by over 15,000 readers a months (and rapidly growing!!) and the individual will receive a pair of Vibram FiveFingers of their choice.
The deadline for all stories is friday May 24th.
Guidlines:
1. Tell your story.
There is no specific length or number of words. If it helped you, it may help someone else so don’t leave out the details!!
2. Everyone likes pictures.
Send as many as you would like! If you have X-rays, MRIs, CTs, Bone scans, send images! Race photos, picture or your race medals or bibs, SEND THEM! Pictures of your feet are also ideal!!
3. Include the following:
Full Name (it will not be included in post)
Age:
Location:
Thanks! We look forward to reading everyone’s stories!!!
Submit your story by clicking here. (or email to drnickcontest1@gmail.com)

A new study accepted for publication in Arthritis & Rheumatism has demonstrated reduction in the force through the knee joints as well as pain when the patients were either barefoot or wearing minimalist shoes which closely mimics the gait of someone walking barefoot. This article is greatly needed in the world of orthopedics where the majority of surgeons are still prescribing foot orthotics to treat many of the lower extremity injuries that do not warrant surgery. Despite the fact that literature does not support the use of foot orthotics for conditions such as plantar fasciitis, shin splints, knee pain, IT band syndrome, piriformis syndrome, and many other running injuries, our society still sees an overwhelming number of physicians and health care providers implementing them.
Why orthotics are over utilized is a tough question to answer. For years they were prescribed to prevent excessive pronation which was thought to be a biomechanical fault in individuals leading to injuries. This continues to be an indication for use, although excessive pronation is not as detrimental as we once thought. Many times it becomes nothing more then convenience for a physician to prescribe an orthotic for a patient with unexplained foot pain with no real clinical explanation. In my practice, these patients tend to show up with bags of shoes and orthotics with continued pain.

This recent article acknowledges that recent studies have demonstrated both barefoot walking as well as walking in a minimalist shoe is associated with reductions in knee loading compared to conventional footwear. The primary focus of this article was to demonstrate a reduction force to the medial knee as well as decreased in symptoms knee OA over a longer period of time which in this case was 6 months. Scientifically the study looked at peak external knee adduction moment and adduction angular impulse. Both parameters reflect the extent of medial compartment knee loading during walking. The results demonstrated a 19% reduction if the force to the medial knee as well as a reduction in pain by 36%.
In my opinion this is extremely significant because this is a relatively long term study combined with previous research that demonstrates decreased force to the knee joints as well as pain as a result of functioning in less of a shoe. So we see here the medical literature since at least 2006 has been evaluating the body’s (specifically the knee) response to functioning barefoot, in minimalist shoes, and traditional shoe gear. It will take time to see the effects of these as well as future studies to make there way to actual medical practices, especially the orthopedic and podiatric specialties that focus more on surgical therapy then “running form” and “technique”. Remember that for the past 40 or so years these specialities have believed in and recommended countless amounts of orthotic devices to their patients as well as taught this philosophy to students and residents. Industries have evolved where the primary focus is manufacturing foot orthotics that are custom made for the patients feet. It has become common place for specialty shoe stores to recommend over the counter inserts as an adjunct to the traditional running shoe being sold to their customers. Our society has accepted that we need to “support” our feet and arches. As you can imagine it is going to be very difficult, as well as timely, to see such a drastic change occur to where we will see the standard of care move from supportive running shoes and orthotic devices to more minimalist style footwear. The change is beginning to occur though as evident by the focus of current research as well as the evolution of more minimalist shoe gear. Over the past several years heel height has decreased from an average of 12mm to 8mm. More then likely, the change is going to occur in the running and shoe industry first before it makes its way to the medical community. Why? We have already seen this happen with today’s current standard of care. The paradigm for recommending shoe-gear that physicians follow today evolved from the shoe industry.

So what shoes does Dr. Nick run in? I tend to train in many different shoes as a result of being able to test products and give my opinion on them. But what did I pick to run my recent marathon in? The New Balance RC5000. This was the first marathon I had done in since transitioning to minimalist shoes 4 years ago and I put a lot of thought into choosing this type of shoe. It is a racing flat but this had nothing to do with my choice – I’m not an elite marathoner!! In fact, I was even questioned about them after the race by the man who won with a time of 2:30. He had never seen them before. After explaining that they are “racing flats” but I’m not racing, he agreed “what ever works for you!”
Choosing this shoe.
Okay. You have to remember, the last marathon I ran I was wearing The Asics Gel Kayano and had not even had a thought about minimalist shoes. This was in 2005 and it would take me roughly 3 more years of understanding how these shoes were not working and how I should be running. The majority of my miles over the past 3 years have been in FiveFingers. My treadmill runs are always barefoot (unless I’m doing a tempo run) and occasionally I’ll do a barefoot run outside. I had run my last half marathon very comfortably with a 7:43 pace in a pair of New Balance Minimus Zero Road shoes. For a distance of 26.2 miles, I wanted a bit of cushion that I could more or less use to “cheat”. Meaning as your muscles tire toward the end, that small amount of cushion helps with the pounding but still let’s your foot feel the ground and not interfere with your form. The RC5000 was perfect. It weighs 3.3 oz (lightest shoe I own) and has a 4mm heel drop. The 4mm heel drop is something I’m not used to as all of my training shoes are flat, or zero drop. It worked great. I could feel the height difference but it was pleasant to have at miles 20 and up when the eccentric contractions of the calf musculature are fighting to lower the heel to the ground. It softened the heel landing at that point of the run. I do think anything higher would have positioned my foot in a manner that would have compromised my form.

The shoe itself has a small amount of cushion to the entire sole, but still allows you to feel the ground (see full review here). The tread is very minimal (basically just little soft rubber spikes) but surprisingly it didn’t wear down much! I didn’t train much in his shoe so that I could save its life for the marathon. I did several tempos in it to get used to the feel. Not sure I’d recommend it for everyday miles, but it was a perfect shoe for a marathon or half marathon in my opinion.
I had no issues with my feet at the end of the race. My forefoot/metatarsal heads were not sore in the least bit and I had no arch soreness. In fact, at miles 20 and up when everything starts to tire, my feet were the farthest from my mind as they felt great! Even the day after the race I had absolutely zero soreness to my feet, arches or heels. Of course I have prepared my feet strength-wise over the past several years through the many miles I have logged in minimalist shoes so I can’t give all the credit to the shoes. Having said that, they were the perfect choice for me!


Part 1: Lets Get Started
This series is intended for someone who has never ran before, someone who wants to get back in running after being inactive for a period of time, or someone needs to reset their running.
What most people who have never ran seriously before don’t realize is they don’t need to “kill themselves” with each run. Even the elite marathoners do not run every run hard. 80% of your weekly mileage should be at an easy pace, and this is only if you are training for a race. If you are just starting out or building a base, then all of your runs should be at an easy pace. What defines an easy pace? It should be conversational. Meaning you should be able to carry an entire conversation without stopping to take a breath. A more scientific way is to wear a heart rate monitor and run at your “aerobic rate”. This can be found by subtracting your age from 180 and was established by Dr. Phil Maffetone. Maffetone trained many elite athletes and even helped Mark Allen win six Ironman Events, with the last being at age 37! For example, a 35 year old would be training at a heart rate of 145 or lower on all of their easy runs regardless of the pace. This will help build ones aerobic fitness and eventually their pace will improve but at the same heart rate. So one may be running at a 10:00 to 10:30 mile pace beginning this type of training, and by 4-6 months into it they may be running 9:30 to 10:00 miles at the same pace.
Several things to consider
Beginning Runners
Do not let speed or pace deter you from running, regardless of what pace your fellow runners may be running. Your goal is to keep your heart rate in the appropriate zone. If this means walking, then you need to walk. Walk 2 minutes, then run 2 minutes. Focus on your hear rate and eventually you we will be running more then waking. Start of with 30 minutes of activity and progress to one hour. You will first obtain 30 minutes while running them progress to longer activity. Remember, your goal is not to see how fast or far you an run, but rather to sustain your heart rate in its aerobic zone for up to sixty minutes. This will build cardiovascular endurance making you a better runner, as well burn more fat. The ability to burn fat while running slow is a topic for another discussion but one will burn more fat running slower then harder.
Seasoned Runners
As many runners head out the door, they have a predetermined pace before they even start their run. This can be problematic because pace is not a true determinant for gauging how “hard” you should be running. By using the “no pain – no gain” philosophy, your body becomes vulnerable to overuse and eventually can become injured. Many runners have a goal of becoming faster and think they need to run faster to accomplish the. This is definitely NOT TRUE! I have made this mistake and have also witnessed countless runners do the same. Slow down! I have seen runners PR in a 5k by simply adding mileage and slowing there pace down to an aerobic pace. If you are reading this and currently have been running half marathons or marathons and just can’t improve your time regardless of how fast and how many 800 and mile repeats you are doing- I suggest you slow down. Slowing down and running at your aerobic pace will improve your efficiency in 3-6 months. While this may seem like a long time, it is not. I tell many of my runners that the most important part of any marathon training program is the 6 months leading up to it.
Answers to questions you may have from what I has been discussed here can be found in most of my blog posts. If you want to ask a question, please feel free to do so in the comments below and I’ll do my best to answer all of them. Try tweeting me as well! If I’m in between patients you may get a quicker response!! @runnerdoctor

Just an interesting article I stumbled upon and thought everyone might enjoy….
(Photo: ABCnews.go.com)
Running used to come with street cred. You got the head-clearing glory of those pre-dawn miles and plenty of fitness prowess was conferred upon you for it. Now, it seems everyone who laces up their sneakers is upping the ante and training for a full-blown marathon. When did running 26.2 miles become the brass ring of fitness? And should it be?
“I feel like everybody does marathons now,” observes Jess Underhill, a New York City runner, coach, and founder of Race Pace Wellness. “Most of my clients are working towards marathons, and if they’re not, they’re on the fence about it.” If you’re a runner, you’re a potential marathoner, the thinking goes.
The numbers reflect that sentiment. According to Running USA, in 1980, 143,000 people finished marathons in the United States; in 2011, that number rose to 518,000. In New York, about 15,500 more pavement-pounders finished the ING New York City Marathon in 2011 than 10 years earlier. And while the country debuted 550 new marathons between 2000 and 2012, getting a spot in one is often like trying to score a ticket to see Lady Gaga at MSG.

“There’s a stigma now if you’re a runner and you haven’t done a marathon. People that aren’t running marathons feel inferior,” says Jess Underhill.
As more and more people cross the finish line, median times are getting slower. “In the past, it was more hard-core, serious runners finishing marathons,” explains New York Road Runners chief coach John Honerkamp. “Now, it’s the masses. It’s a bucket list item.”
THE SHIFT
So how did the marathon of elite athletes become the brass ring of bar-stool bragging rights for the rest of us?
Of course, general interest in running as a sport and social past-time has been increasing, and the masses of people taking it up (especially women, who were barely represented in the sport as recently as the ’80s and now outnumber men) want to have something to work towards.
More specifically, runners and coaches tend to point to the growth of charities using the races as fundraising tools. “It increases the accessibility of the races and markets them to people,” says Meghan Reynolds, who co-owns Hot Bird Running with Jessica Green. “Everyone wants to do good, and this way you can give to charity and do something good for yourself.”
And, of course, there’s a cool-kids-club effect. “People are inspired by their friends and family who’ve completed marathons,” Underhill explains. “They think ‘Well, if Sally can do it, I can do it.’”

“If you want to become a long-distance runner and continue to run, you shouldn’t always be in marathon training,” say Meghan Reynolds and Jessica Green.
THE DOWNSIDE?
The positive effects of the marathon boom are obvious—lots of people setting tough goals for themselves, meeting challenges while getting healthy and fit, and building community. But is there a downside?
“Some people run their first road race as a marathon, and I think that’s crazy,” says Honerkamp, who recommends starting with a race like a 5K and gradually increasing your race distance as you become more experienced.
Most seasoned runners and coaches agree, because running newbies tend to underestimate the stress the training will put on their bodies and don’t spend the time to build mileage gradually in a smart, safe way.
Reynolds and Green say that many of their clients come to them because they tried to train on their own, or too quickly, and were injured. “We believe everyone can run and achieve that distance, but it’s a lot on your body. We always say, ‘You have to respect the distance!’” —Lisa Elaine Held
Article originally appeared at:
Tapering? Wrap It Up With a Burst
In the days before a race, scale back on mileage but not instensity.
In principle, tapering should be simple–run less so you’re rested for race day. In practice, many athletes find two to three weeks of cutting back on mileage and intensity makes their legs feel heavy and lifeless. But Spanish coach and physiologist Iñigo Mujika, a leading expert on tapering, sees a way around that problem. Mujika suggests athletes start their taper early, scaling back on mileage but not intensity, then three days before the event, “reload” their muscles with an interval workout. Performing these workouts when your legs are fresher than they’ve been for months can actually increase your fitness.
Indeed, too much rest or slow running lowers the muscle tension in your legs, says Norwegian Olympian and 13:06 5-K runner Marius Bakken, which is why they feel flat and sluggish. Short, fast bursts of running raise muscle tension back up. If you get your taper right, your body will respond by producing more oxygen-carrying red blood cells, lowering stress hormone levels, and storing more fuel in your muscles–enough to shave about three percent off your finishing time, on average. Here’s how to inject some energy into your taper so you shed fatigue and sharpen your edge.
Plan it: For a marathon, cut mileage to 80 to 90 percent of normal three weeks out; reduce to 60 to 70 percent two weeks out, and 50 percent in the final week. Maintaining intensity is crucial to avoid losing fitness, so don’t slow your easy runs down; for hard workouts, do fewer intervals than you normally would but run them at your usual pace. Stick to one day off: The volume reduction should come from shorter, not fewer, runs. If you’re racing a 5-K or 10-K, reduce the length of your runs so your total mileage the week before race day is about half of your typical number.
Reload it: In the final week, for a Sunday race, take a rest day on Wednesday. Over the next three days, reload by running an interval workout at goal pace, an easy run, and an easy run with strides. For your interval run, simply modify sessions that you’ve been doing all along and resist the temptation to blast repeats faster than usual because your legs are fresh. The easy runs serve to get your legs back into the rhythm and feel of running. Aim to run at your usual pace for half your typical easy-run length, but if your legs feel heavy, add an extra mile and pick up the pace toward the end.
Turn It Up
A reload plan for the last few days before your big event
Wednesday
Marathon reload: Off
5-K or 10-K reload: Off
Thursday
Marathon reload: 2 x 1 mile at marathon pace with 2:00 rest; 4 x 400 at 10-K pace with 90 seconds rest
5-K or 10-K reload: 800 meters at 10-K pace; rest 45 seconds; 300 meters at 5-K pace; rest 2:00. Repeat sequence three times.
Friday
Marathon reload: 4 miles easy
5-K or 10-K reload: 4 miles easy
Saturday
Marathon reload: 4 miles easy; 4 x 30-second strides at 10-K to half-marathon race pace
5-K or 10-K reload: 3 miles easy; 5 x 100 meters at mile to 5-K pace
Sunday
Marathon reload: 26.2
5-K or 10-K reload: 5-K or 10-K

The first issue of the Natural Born Runner Magazine out of the UK is hitting the shelves this month. This is the first magazine dedicated to natural/minimalist/barefoot running. I am very excited to be a member of the editorial panel along with Daniel Leiberman, Irene Davis, Mark Cucuzzella, and other great researchers and runners. You can read a PDF of the first magazine online here. I have also posted my article below. Enjoy!
TREATING RUNNING INJURIES: FORM VS FOOTWEAR
Running injuries can be very frustrating for physicians, as such injuries can be extremely time consuming and the stereotypical runner will not curtail running to resolve an injury. If you tell a runner not to run, most of the time he or she will not listen to you and not follow through with your prescribed treatment regimen. This challenge leads many physicians to not treat runners. Added to this frustration is the recommendation of shoe gear. Whether someone has been running for many years or is just starting out, he or she will tend to place a lot of emphasis on what shoes to wear. Form is traditionally ignored. Runners, as well as practitioners, will typically make a change their shoes in an attempt to fix an injury.
What most practitioners do not realise is that there is no evidence-based literature on recommending a running shoe to prevent or reduce injury (Footnotes 1 to 8).
Following the popular paradigm of recommending a running shoe based on foot type leads to frustration, as numerous models are introduced frequently. Not only does this complicate matters, but when we analyse the reasons that we use a particular shoe, the situation becomes even more blurred.
There exists no clear scientific basis for using one particular shoe model over another for given foot types or pathologies, despite what some manufacturers claim (1). The term ‘appropriate shoe’ is a misnomer when judged by the outdated paradigm of selecting a shoe according to arch type, yet many still advocate shoes this way. Even the implementation of orthotics has little if any bearing on reducing or correcting injuries in runners (9 to 12).
We also live in a society where some people incorrectly believe they have a flat foot or are over-pronated. Associated with this is the stigma that foot types (especially flat feet) influence injury patterns (13). This, however, is not true (14). Evidence suggests that training patterns actually play more of a role in increasing the incidence of running injuries (15 and 16). The key is understanding that form and training patterns play more of a role in improving one’s running and at the same time reducing injury (17).
Before seeking treatment for an injury, most runners will run through the pain, thinking that it will eventually resolve itself. When the pain finally becomes too severe to allow the runner to continue, medical advice is usually sought.
The standard protocol for a physician or sports medicine specialist treating a runner is as follows: 1) Ask the athlete how many miles a week he or she is running. 2) Evaluate shoe gear. 3) Find out the number of miles on the current shoe gear. 4) Carry out a biomechanical assessment of the feet and lower extremities. If the runner is seen in a more specialised clinic, gait analysis is sometimes performed. Overpronation is commonly diagnosed and an effort to control this excessive motion is usually attempted with orthotics. High-tech scans and pressure analysis may also be performed, although very little if any applicable information can be generated from this.
Form analysis, on the contrary, focuses more on the runner’s style with respect to foot strike, cadence and the runner’s overall body posture. Form analysis is slowly becoming a panacea to help improve someone’s running and reduce or resolve injuries (17 and 18). Runners tend to develop injuries as a result of poor or incorrect form and overuse, which many times overlap (15 and 19). Debate exists as to what is the ‘proper form’ for running. Proper form will certainly vary from one runner to the next, making each runner’s form ‘ideal’ for him or her. There are, however, certain aspects of form a runner should strive to attain: adequate foot strike, cadence and posture.
FOOT STRIKE
Foot strike is the first aspect that needs to be addressed. There exists a common misunderstandings hat all aspects of gait, whether walking or running, should begin with a heel strike. Following heel strike, the force is carried toward the outside edge of the foot and then moves inward to the great toe joint. There, a large amount of force is created to propel the body forward. Much of this is attributed to Root et al, in their discussion of walking mechanics, which over the years has somehow carried over to running (20). The practitioner sometimes will examine the shoe gear to see if any wear patterns exists that would indicate increased pronation, as indicated by wear seen more on the inside of the heel than on the outside.
The problem with this pathway is that we have no evidence- based studies to indicate that heel striking is the correct way to land when running. In fact, recent studies demonstrate higher injuries amongst collegiate cross-country runners that heel strike than among those who forefoot strike (21 and 22).
Numerous studies have compared shod and unshod runners and a forefoot strike pattern is adapted among those who run without shoes (23 to 27). We all see that elite runners tend to forefoot strike more than slower recreational runners, as demonstrated by Larson et al (28 and 29). Evidence exists that the human body has a natural tendency to forefoot or midfoot strike when running barefoot or in minimalist shoes (23 and 26).
Heel strike vs forefoot/midfoot strike
By striking the ground with the heel first, the rear foot joints and ankle take the brunt of the force, which overuses the lower leg muscles, leading to injuries such as severe tendonitis or conditions commonly called ‘shin splints’. We also see that during a rearfoot strike, the forefoot (including the toes) and midfoot joints really serve no purpose in absorbing shock. If, instead, we use these joints with a forefoot or midfoot strike, the entire foot can work to absorb shock, as opposed to only the rear foot joints and leg (30). When we forefoot or midfoot strike, we can control the amount of pronation innately by activating our leg musculature.
Consider that one common complaint of those who make the transition to minimalist shoes is ‘calf pain’. This is due to the activation of the calf muscles in efforts to slow the heel from striking the ground. They are contracting eccentrically to ‘slow’ pronation. This does not need to be scientifically demonstrated in future studies, as we already know that if pronation of the foot is dorsiflexion, eversion and abduction, then these muscles collectively are contracting as they are lengthening in order to ‘slow’ pronation. As they become strong enough, they will control the pronation that occurs during foot strike (31 and 32).
RUNNING SHOES
Examining the categories of traditional running shoes reveals that manufacturers have created them according to three foot types: flat foot, normal arch, and high arch. The American Academy of Podiatric Sports Medicine (AAPSM) has defined the categories as maximum stability, stability, and neutral. For example, ASICS defines its stability category shoe as “structured cushioning” (33). According to ASICS, “the structured cushioning segment is designed for runners who pronate slightly more than normal and generally have a normal arch” (33). This infers that the runner is heel-striking. Otherwise, why would there be a need to control motion? Some of the normal pronation that is encountered when a runner forefoot or midfoot strikes could be inhibited by this motion-controlling apparatus.
Why then are running shoes created with a thick cushioned heel and motion control support? That question is debatable, but it is clear that as running shoes have evolved over the past 40 years, we have seen no reduction in injury rates and marathon times have remained largely unchanged. Many physicians still abide by the rule of changing your shoes every 300 to 500 miles. This became popular after a 1984 study that demonstrated shock absorption loss after 250 to 500 miles of running (34). Since then, studies have demonstrated that as absorptive qualities of a shoe are lost, the foot becomes more stable, leading to the likelihood of reduced injury with greater mileage (35, 36 and 37).
At the same time, a notion that runners “need a great deal of shock attenuation because they don’t absorb shock naturally through pronation” implies that we need to pronate to absorb shock. It becomes extremely crucial to look at pronation in terms of the entire foot, as opposed to only the subtalar joint, because more shock attenuation can be achieved using the forefoot and midfoot.
Even if we consider implementing an orthotic into the shoe to control pronation, we have to consider the purpose of doing this. The orthotic for an overpronator is typically designed to control motion at the subtalar joint that results in the increased pronation. With forefoot striking, we have to look at this from an entirely different perspective, in which the orthotic would not serve the same purpose; therefore, its use is of question.
LANDING
Where the foot strikes in relation to the rest of the body is also crucial. To increase efficiency and reduce shock to the lower extremity, the foot should be landing under the body’s centre of gravity, or close to it. This engages the body’s natural spring mechanism by using eccentric contractions of the muscles at the ankle, knee, and hip, during landing. In contrast, heel striking, with the leg reaching in front of the body’s centre of gravity, results in the leg impacting in an extended position, increasing the force to these joints. Even if one heel strikes with the foot below the centre of gravity, you will lose part of the spring as the reduction of direct force by its conversion to rotational force through the ankle is lost.
CADENCE
Cadence is another piece of the puzzle. Cadence is the number of steps a runner takes per minute. Examining elite runners and marathoners has determined that achieving a cadenceof 180 steps per minute or higher will result in increased efficiency (38). Running with a forefoot strike pattern makes it easier for one to increase the cadence (23). This high cadence keeps the runner closer to the ground, reducing the vertical motion associated with increased impact forces (23). Shorter strides are associated with a higher cadence, but as speed increases, the stride length will also increase (23, 27 and 32). It is important to understand that cadence should not vary with speed. For example, if running a 10-minute mile or slower, your cadence should remain at 180 or above. Faster paces, such as five to six minutes per mile, can sometimes reach cadences of 200 or above. The key is to understand shorter strides; faster turnover will increase efficiency and reduce ground reactive forces.
POSTURE
Finally, the body’s overall posture also needs to be assessed. This can be somewhat confusing, because some running instructors advise maintaining an upright posture, while others advise leaning forward. Both are actually correct. The body’s overall position should be erect, but it should be falling forward. ‘Leaning’ should not occur at the waist, as it does in bending over, but the entire body should be angled forward. Running in place and then leaning forward to begin movement will help to teach this concept. This increases efficiency by using forward momentum, as opposed to decelerating with each step, which recruits greater musculature.
CONCLUSION
Focusing on the matters discussed will help to improve a runner’s efficiency, leading to reduced injury. New Balance has partnered with Kurt Munson, a well-known running shoe retailer from Michigan, to create the educational concept known as Good Form Running (18), which teaches these steps in a simplistic manner. Speciality running shoe stores across the United States are holding clinics to teach this method.
Interestingly, children tend to run this way when they are unshod and playing outside (39, 40 and 41). The younger they are, the more noticeable this is, as their gait has not been altered by wearing shoe gear. As for paediatric shoes, the American Academy of Pediatrics recommends not wearing shoes until it is required by the environment (42). This helps to encourage natural foot motion, thereby enabling adequate development and strength gains.
A final point it is crucial to mention is training patterns. Most recreational runners and even elite runners tend to train too hard (17). Improving the body’s aerobic capacity means continuously training at an aerobic rate (ibid). This is best achieved through the use of a heart rate monitor. Training too much at too high a heart rate can lead to overuse injuries (ibid). Runners too often focus on maintaining a pace instead of listening to their body and their training becomes borderline anaerobic (ibid).
Obviously, there is more to running than has been discussed here, but having this as a foundation really helps anyone just starting to run, or even those who have been running for many years. It is crucial for physicians treating running injuries to understand this.
In conclusion, it seems that most practitioners are straying from the path of helping a runner by focusing on shoes, as opposed to form. The term ‘appropriate shoe’ is a misnomer when viewed through the old paradigm of selecting a shoe according to arch type, yet many still advocate choosing shoes this way. Running should allow the foot to function as it was designed to: naturally, without inhibiting motion. Adding cushioned heels and motion control mechanisms can inhibit this.
By viewing shoes as the first line of treatment for most conditions, we must make sure they do not interfere with the foot’s natural function. The shoe should feel comfortable initially (not with time), without a need for the foot to ‘get used to the pressure pushing against the arch’. A gradual adaptation to this way of running is obviously needed, or injury can result, as our feet and bodies may have been accustomed to a different form and supportive shoe. The approach is very similar to creating a programme for someone just beginning to run, although more gradual.
MINIMALIST FOOTWEAR IS NEITHER A FAD
NOR A GIMMICK.
Think about sports specificity. We train in a heavy cushioned shoe with an elevated heel that puts our body in an abnormal position; then, when it comes time to race, we remove
it. There’s not much logic behind that. As athletic trainers, we always put our athletes through a battery of tests to make sure they are ready for competition. These involve activity done the way it would be performed in the event. The logic behind not strengthening
the foot by ‘casting’ it with a motion control shoe and heel striking makes no sense.
As for the surge in injuries that practitioners are claiming to see from runners wearing minimalist shoes, it’s due to the training regimen and form. Shoes do not directly create injury. As for overweight people, or those with poor biomechanics using them, being overweight and heel striking certainly is illogical when compared to reducing shock by forefoot striking and obtaining proper form. The same is true for those with poor biomechanics. Remember we have to redefine ‘poor biomechanics’, because when you forefoot strike, what we learned from Root in terms of overpronation no longer applies.
Shoes with a heel lift for plantar fasciitis work against the stretching that has been advocated in increasing ROM at the ankle joint. Consider that by placing a patient in a 14mm-drop shoe, we actually induce an equinus deformity and then tell the patient to function in it all day.
FOOTNOTES
1. Knapik J.J., Trone D.W., Swedler D.I., villasenor A., Bullock S.H., Schmied E., Bockelman T., Han P., Jones B.H.: Injury reduction effectiveness of assigning running shoes based on plantar shape in Marine Corps basic training. Am. J. Sports Med. 2010 Sep; 38(9):1759-67. Epub 2010 June 24.
2. Clinghan R., Arnold G.P., Drew T.S., Cochrane L.A., Abboud R.J.: Do you get value for money when you buy an expensive pair of running shoes? Br. J. Sports Med. 2008 Mar; 42(3):189-93. Epub 2007 oct. 11.
3. Butler R.J., Hamill J., Davis I.: Effect of footwear on high and low arched runners’ mechanics during a prolonged run. Gait Posture. 2007 Jul; 26(2):219-25. Epub 2006 oct. 20.
4. Kerr R., Arnold G.P., Drew T.S., Cochrane L.A., Abboud R.J.: Shoes influence lower limb muscle activity and may predispose the wearer to lateral ankle ligament injury. J. orthop Res. 2009 Mar; 27(3):318-24.
5. Marti, B. (1998): Relationships between running injuries and running shoes — results of a study of 5,000 participants of a 16K run. The Shoe in Sport. Chicago: Year Book Medical Publishers. 256–265.
6. Herzog W.: Running injuries: is it a question of evolution, form, tissue properties, mileage, or shoes? Exerc. Sport Sci. Rev. 2012 Apr; 40(2):59-60. Yeung S.S., Yeung E.W., Gillespie L.D.: Interventions for preventing lower limb soft-tissue running injuries. Cochrane Database Syst. Rev. 2011 Jul 6; (7):CD001256. Review.
7. Yeung S.S., Yeung E.W., Gillespie L.D.: Interventions for preventing lower limb soft-tissue running injuries. Cochrane Database Syst. Rev. 2011 Jul 6; (7).
8. Clinghan R., Arnold G.P., Drew T.S., Cochrane L.A., Abboud R.J.: Do you get value for money when you buy an expensive pair of running shoes? Br. J. Sports Med. 2008 Mar; 42(3):189-93. Epub 2007 oct. 11. PubMed PMID: 17932096.
9. Gross M.L., Napoli R.C.: Treatment of lower extremity injuries with orthotic shoe inserts. An overview. Sports Med. 1993; 15(1):66-70.
10. Stackhouse C.L., Davis I.M., Hamill J.: orthotic intervention in forefoot and rearfoot strike running patterns. Clin. Biomech. (Bristol, Avon). 2004; 19(1):64-70.
11. Mattila v.M., Sillanpää P.J., Salo T., Laine H.J., Mäenpää H., Pihlajamäki H.: Can orthotic insoles prevent lower limb overuse injuries? A randomised-controlled trial of 228 subjects. Scand. J. Med. Sci. Sports. 2011 Dec; 21(6):804-8. doi: 10.1111/j.1600-0838.2010.01116.x. Epub 2010 May 12.
12. Kilmartin T.E., Wallace W.A.: The scientific basis for the use of biomechanical foot orthoses in the treatment of lower limb sports injuries — a review of the literature. Br. J. Sports Med. 1994; 28(3):180-4.
13. Hohmann E., Reaburn P., Imhoff A.: Runners’ knowledge of their foot type: do they really know? Foot (Edinb.). 2012 Sep; 22(3):205-10. doi: 10.1016/j.foot.2012.04.008. Epub 2012 May 18. 14. Michelson J.D., Durant D.M., McFarland E.: Injury risk associated with pes planus in athletes. Foot Ankle Int. 2003; 23(7):629–933.
15. Hespanhol Junior L.C., Costa L.o., Carvalho A.C., Lopes A.D.: A description of training characteristics and its association with previous musculoskeletal injuries in recreational runners: a cross-sectional study. Rev Bras Fisioter. 2012 Jan.-Feb.; 16(1):46-53.
16. van Gent R.N., Siem D., van Middelkoop M., van os A.G., Bierma-Zeinstra S.M., Koes B.W.: Incidence and determinants of lower extremity running injuries in long distance runners: a systematic review. Br. J. Sports Med. 2007 Aug; 41(8):469-80; discussion 480. Epub 2007 May 1. Review.
17. Maffetone, Philip. The Big Book of Endurance Training and Racing. Skyhorse Publishing. 2010 Sep. 22.
18. http://www.goodformrunning.com.
19. Edwards W.B., Taylor D., Rudolphi T.J., Gillette J.C., Derrick T.R.: Effects of stride length and running mileage on a probabilistic stress fracture model. Med. Sci. Sports Exerc. 2009 Dec.; 41(12):2177-84.
20. Root M.L., orien W.P., Weed J.H.: Normal and Abnormal Function of the Foot – volume 2. Clinical Biomechanics Corp., Los Angeles, CA, 1977.
21. Goss D.L., Gross M.T.: Relationships Among Self-reported Shoe Type, Footstrike Pattern, and Injury Incidence. US Army Med. Dep. J. 2012 oct.-Dec.: 25-30.
22. Daoud A.I., Geissler G.J., Wang F., Saretsky J., Daoud Y.A., Lieberman D.E.: Foot strike and injury rates in endurance runners: a retrospective study. Med. Sci. Sports Exerc. 2012 Jul.; 44(7):1325-34.
23. Lieberman D.E., venkadesan M., Werbel W.A., Daoud A.I., D’Andrea S., Davis I.S., Mang’eni R.o., Pitsiladis Y.: Foot strike patterns and collision forces in habitually barefoot versus shod runners. Nature. 2010 Jan. 28; 463(7280):531-5.
24. Morley J.B., Decker L.M., Dierks T., Blanke D., French J.A., Stergiou N.: Effects of varying amounts of pronation on the mediolateral ground reaction forces during barefoot versus shod running. J. Appl Biomech. 2010 May; 26(2):205-14.
25. Eslami M., Begon M., Farahpour N., Allard P.: Forefoot-rearfoot coupling patterns and tibial internal rotation during stance phase of barefoot versus shod running. Clin. Biomech. (Bristol, Avon). 2007 Jan; 22(1):74-80. Epub 2006 oct. 17.
26. De Wit B., De Clercq D., Aerts P.: Biomechanical analysis of the stance phase during barefoot and shod running. J. Biomech. 2000 Mar.; 33(3):269-78.
27. Robbins S.E., Hanna A.M.: Running-related injury prevention through barefoot adaptations. Med. Sci. Sports Exerc. 1987 Apr.; 19(2):148-56.
28. Larson P., Higgins E., Kaminski J., Decker T., Preble J., Lyons D., McIntyre K., Normile A.: J. Sports Sci. 2011 Dec.; 29(15):1665-73. Epub 2011 Nov. 18.
29. Hayes P., Caplan N.: Foot strike patterns and ground contact times during high-calibre middle-distance races. J. Sports Sci. 2012; 30(12):1275-83. doi: 10.1080/02640414.2012.707326. Epub 2012 Aug. 2.
30. Nigg B.M.: The role of impact forces and foot pronation: a new paradigm. Clin. J. Sport Med. 2001 Jan.; 11(1):2-9. Review.
31. Feltner M.E., MacRae H.S., MacRae P.G., Turner N.S., Hartman C.A., Summers M.L., Welch M.D.: Strength training effects on rearfoot motion in running. Med. Sci. Sports Exerc. 1994 Aug.; 26(8):1021-7.
32. Ardigò L.P., Lafortuna C., Minetti A.E., Mognoni P., Saibene F.: Metabolic and mechanical aspects of foot landing type, forefoot and rearfoot strike, in human running. Acta Physiol Scand. 1995 Sep.; 155(1):17-22.
33. http://www.asicsamerica.com/Shoe-Fit-Guide/.
34. Cook S.D., Kester M.A., Brunet M.E.: Shock absorption characteristics of running shoes. Am. J. Sports Med. 1985 Jul.-Aug.; 13(4):248-53.
35. Kong P.W., Candelaria N.G., Smith D.R.: Running in new and worn shoes: a comparison of three types of cushioning footwear. Br. J. Sports Med. 2009 oct; 43(10):745-9. Epub 2008 Sep. 18. 36. Hamill J., Bates B.T.: A kinetic evaluation of the effects of in vivo loading on running shoes. J. orthop. Sports Phys. Ther. 1988; 10(2):47-53.
37. Rethnam U., Makwana N.: Are old running shoes detrimental to your feet? A pedobarographic study. BMC Res. Notes. 2011 Aug. 24; 4:307.
38. J. Daniels’ Running Formula. Champaign, IL: Human Kinetics, 2005.
39. Wolf S., Simon J., Patikas D., Schuster W., Armbrust P., Döderlein L.: Foot motion in children shoes: a comparison of barefoot walking with shod walking in conventional and flexible shoes. Gait Posture. 2008 Jan.; 27(1):51-9. Epub 2007 Mar. 13.
40. Wegener C., Hunt A.E., vanwanseele B., Burns J., Smith R.M.: Effect of children’s shoes on gait: a systematic review and meta-analysis. J. Foot Ankle Res. 2011 Jan; 4:3.
41. Wolf S., Simon J, Patikas D., Schuster W., Armbrust P., Döderlein L.: Foot motion in children shoes: a comparison of barefoot walking with shod walking in conventional and flexible shoes. Gait Posture. 2008; 27(1): 51-9.
42. Hoekelman R.A., Chianese, M.J. Presenting Signs and Symptoms. In: McInerny T.K., Adam H.M., Campbell D.E. (eds.) American Academy of Pediatrics Textbook of Pediatric Care, 5th edition, American Academy of Pediatrics, Elk Grove village, IL, 2.

Below is an article from World Magazine where myself Dr. Mark Cuccuzzella, MD were interviewed by Caroline Leal. Great read!
Footloose and shoe free
Originally appeared at http://www.worldmag.com/2013/04/footloose_and_shoe_free
Four times a week—after leaving work from a law firm in downtown Austin, Texas—Jacob Aschmutat kicks off his dress shoes, slips on a pair of Vibram FiveFingers and runs for up to 6 miles on sidewalks and biking trails. Although his feet are technically covered, Aschmutat feels like he’s barefoot, the purest form of running, according to enthusiasts.
In 2009, Christopher McDougall’s bestseller Born to Run, widely credited with sparking the barefoot running trend in the Western World, inspired many converts to adopt a shoeless stride. The book focuses on a Mexican Indian tribe whose members run painlessly for long distances in little more than sandals. Some devotees claim running unshod makes them less prone to injury, and is more natural and comfortable overall. Although they represent a minority of runners, the ranks of barefoot runners have grown steadily in recent years.
But despite the popularity of barefoot running, abandoning shoes completely isn’t an option for scores of runners who train on urban streets or rocky trails. Americans reportedly spent $59 million on “barefoot shoes” last year. They rely on footwear like Vibram FiveFingers—the snug, glove-like shoe weighing less than five ounces—to provide adequate protection without detracting from the feeling of running barefoot.
But is minimalist footwear really the healthiest option? A recent study published in Medicine & Science in Sports & Exercise indicates that popular minimalist running shoes, designed to encourage a barefoot running style, are more likely to lead to bone injury. But according to some medical experts, such indications are misleading.
“Shoes do not cause injury,” said Mark Cucuzzella, a physician, minimalist runner and owner of the West Virginia running shoe store, Two Rivers Treads. “Running causes running injury.”
In the recent study, researchers from Brigham Young University looked at 36 experienced recreational runners, all of them wearers of traditional running shoes with no prior experience with “barefoot shoes.” For 10 weeks, 17 participants continued running in traditional shoes, while 19 gradually transitioned to Vibram FiveFingers. Researchers then rated the severity of bone marrow edema, or bone bruising, in the participants’ feet.
MRI scans revealed more than half of those wearing the Vibrams showed signs of bone injuries. These findings support concerns already voiced by others. The New York Times notes “anecdotal evidence, including from physicians who treat runners, indicates that some people who take up barefoot running develop entirely new aches and injuries.”
But the conclusions drawn from such studies are often misleading, Cucuzzella said. He advises runners transitioning from traditional to minimalist shoes to follow the “10 percent rule of exercise,” where runners increase the duration of their exercise in minimalist shoes by 10 percent each week until they are fully acclimated. Barefoot shoe running also has a distinct gait and form—involving a shorter stride, faster cadence and midfoot or forefoot footstrike—that runners must adopt.
Adherence to such protocol seemed absent from the recent study, Cucuzzella said: “The runners in this study followed none of the barefoot training so far as we can tell. If you ask a traditional shod runner to go straight into running in minimal footwear, without strengthening the muscles of the foot or addressing form, you are asking for an injury.”
Cedric Bryant, chief science officer for the American Council on Exercise, stresses that barefoot runners must transition gradually out of traditional shoes and learn the proper forefoot strike pattern through regular practice. “Rather than going out and trying to run your typical distances at your typical speeds, give yourself ample time to adjust to this new style,” he said.
Runner Meagan Wilson of Rochester, New York, learned first-hand that barefoot shoes demand an entirely different approach to foot motion. Hoping to remedy her heel-striking habit, she purchased her first pair of minimalist shoes, a pair of Merrell’s Pace Gloves, but continued running, even upping her mileage, without transitioning gradually or maintaining correct form.
“I wound up shocking my heels and made my Achilles tendons very sore,” said Wilson, who couldn’t run or walk normally for almost three weeks after making the shoe switch. “So the lesson is, ease into running with minimalist shoes and make sure to get proper running form with them before going all out.”
Nick Campitelli is an Ohio podiatrist and marathon runner who has worn Vibrams since 2009. He wears his barefoot shoes not only when running, but also while visiting with patients and working in the operating room. According to Campitelli, the heels on traditional shoes cause wearers to lean back unnaturally, putting stress on their heels and backs. But the heel-free design of barefoot shoes eliminates stress and causes wearers to stand flat on the ground, which is the “most natural and comfortable” position.
“A shoe should allow you to run, not enable you to run,” he said. “Barefoot shoes are ideal in this regard. The only catch is, well, they look weird.”
Campitelli said it’s a “bogus notion” that someone needs a special pair of shoes to run effectively or solve a foot problem. What they need is proper education about foot motion and form, said Campitelli, who believes minimalist shoes should be seen as tools allowing for improved health and exercise, rather than mechanisms capable of preventing or promoting injury by themselves: “It’s not about what you wear, it’s about how you run.”
Copyright © 2013 God’s World Publications. All rights reserved.
Articles may not be reproduced without permission.
Running with sesamoiditis: How I resolved a 10 year injury by ditching my traditional running shoes.
I was asked to discuss this topic from a reader and ironically this is the injury that plagued me for 10 years before I finally learned how to run. Sesamoiditis is a condition where the two small bones of the great toe joint become inflamed. This can be the result of what is termed a bipartite sesamoid bone(referring to two bones that have not united into one during develop) or one that has become fractured. A debate exists amongst the literature as to whether a fracture truly occurs to this bone, and if so can it reunite or heal. Symptoms present with sesamoiditis include pain and swelling to the bottom or plantar aspect of the great toe joint. A sharp piercing feeling is sometimes described and one usually will limp or walk with pressure on the outside (lateral) aspect of the foot to avoid pain. The condition can go on for months and sometimes does not respond to rest or padding. It is very common amongst volley players or sports that entail forceful jumping or exploding off of the ball of the foot.

So here’s my story. I was just starting residency and had ran most of my life at that point. I had done 3 marathons and numerous other types of races and really just ran as a means of relaxation. In the year 2000, I developed pain in my right great toe in the region of my sesamoid bones (for those not understanding what they are, i’ll explain shortly). Initially I attributed it to playing ice hockey and my skates were tight and it placed increased pressure to the great toe joint. The problem was, it never resolved. After living with it for about 4 years, it finally cultivated in the winter of 2003 when I was on a run in the wintery snow of Erie, PA and the pain became so severe I could barely run. I had x-rays taken of my foot and found in addition to the bipartite tibial sesamoid knew I had, I now had a fractured fibular sesamoid to go along with it! I wore a boot for 3 weeks, and had to stop running. It never worked. It calmed it down and eventually I was able to run again, but the pain in this region persisted. I had worn holes out to the great to region in the fabric on the insides of my Birkenstock Clogs that I would operate and work in. Was I putting too much pressure here? I just figured I was limping from the pain and the region was wearing. I continued to run. I would have good months, and bad months. Eventually I went on to run several more half marathons, another full marathon, and other road races. My foot still hurt. I would try multiple custom orthotics, OTC semi-custom orthotics, and even various running shoes, but just couldn’t resolve it. I focused on “heel-striking” because that was what at that time I was “told” was the proper way to run. Imagine my frustration. A podiatrist, foot and ankle surgeon, who couldn’t fix his own foot. I had contemplated have the sesamoid removed but I felt that would be too destructive of a procedure because it is encompassed in the flexor hallucis brevis tendon and would create a ton of scarring and fibrosis. Not to mention that I was still able to run at times with no pain.

Notice the sesamoid on the left (lateral) is in 3 pieces and the sesamoid on the right (tibial) is in 2 pieces. (Dr. Nick’s Sesamoid Bones of right foot)
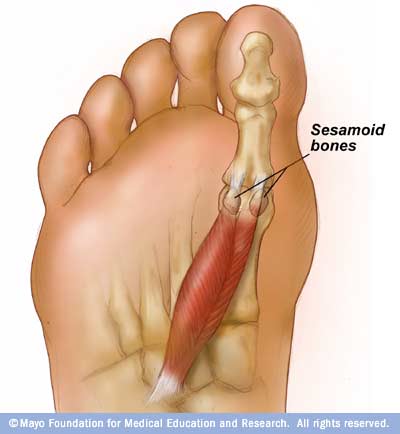
Notice how the sesamoid bones are intratendonous (within the tendon of the flexor hallucis brevis)
Enter 2009, the year when the questions starting pouring in about barefoot running. I was working an event for the Akron Marathon, when the owner of a local running shoe store (Vertical Runner) walked by wearing a pair of FiveFingers. I needed to put them on. I was getting bombarded with questions about them, and what better way then to have them on my feet to draw more attention to the matter. I wore them for the second half of the day with a suit and tie and fielded questions from the manny runners that walked by my booth. By the end of the evening, I had discovered that I was learning to stand differently because these shoes were killing my great toe! How could they possibly be good to run it? But that was just it. They forced me to stand differently. Had I been standing wrong in my other shoes? Absolutely, but I didn’t know it. I was wearing a pair of dress shoes that day, so of course my feet were going to hurt. But what did the shoe have to do withme standing wrong? I didn’t figure this out for at least another year.
I decided to focus a little more on barefoot running then just wearing a pair of FiveFingers. I started pulling the literature to understand this a little better. Surprisingly there wasn’t much out there on barefoot running. In fact most of it was anecdotal by an underground of runners who most would probably laugh at and never think much of it. But there was something about it. They weren’t getting injured and were running this way for years. That’s when I started pulling more and more literature on traditional cushioned running shoes. Surprisingly, there was not a shred of evidence to support prescribing these for running, foot pain, or any foot ailment that I had been treating and recommending them for. While all of this was happening, I had began transitioning to running in my FiveFingers. I will leave that story for another blog post!
After 8 weeksof transitioning, my sesamoiditis was all but gone! I just presumed it was coincidental as I had good months in the past, but never this long. How could this be? The treatment for sesamoiditis is to cushion the 1st MPJ, use a cut out offloading orthotic, or not run at all and rest it. I was, for all intensive purposes, running barefoot and mine resolved! Fast forward 5 months and I now completed a half marathon in a pair of FiveFingers and my sesamoiditis was 100% painfree.
Was it the shoes? Nope. I learned how to run. After another year or more of reading, learning (world wide collaboration of runners and physicians including Mark Cuccuzzella, Dan Lieberman, and Irene Davis) and now lecturing on this fascinating topic, I had finally got it. It has nothing to do with the shoes. It’s how you run. Yes I had strengthened my feet beyond what they had ever been my whole life, but the form I had now grown accustomed to was what was helping me.
So what does this have to do with fixing my sesamoiditis specifically? I took the pressure off of that area. This happened through a multitude of ways, but one that I think is most crucial is eliminating what most podiatrists and biomechanists used to describe as the “propulsion phase” of the gait cycle. By adapting a midfoot/forefoot strike pattern, with shorter strides,and landing with your foot below your body, the force that gets generated to the MPJ is reduced. You no longer pro-pulse with the great toe joint, but instead you drive forward with your thigh and the foot gets picked off the ground. There is a slight push off occurring with the foot, but its through the entire foot, not just the MPJ. So basically instead of pushing off with only your great toe, the entire foot takes the load minimizing the stress to great toe joint. This reduction in stress and force can allow the flexor hallucis longus and brevis tendons in the great toe joint to heal if they were inflamed which we typically refer to as sesamoiditis. This makes the condition more consistent with a tendonitis then a true boney pathology which can explain why many don’t respond to just simply resting the foot.